Training of cervical proprioception in addition to manual therapy
 Isabelle Werner
Isabelle Werner
Neck pain is a common problem, probably increasing today by working with computers, using smartphones and driving (or unfortunately crashing) cars.
What to do, when a patient with unspecific neck pain feels ok after some manual therapy techniques, ergonomic instructions and training of the deep neck flexors, but after two weeks, the same symptoms are back again? Screening of the thoracic spine, first rib, shoulders, TMJ and upper spine show no comparable signs...
Oh, sensorimotor control of the cervical spine is not yet checked! How to test and treat proprioception of the cervical spine? Do our patients have to train the headstand on a wobble board now? Maybe there are some good alternatives! Here some possible answers from articles about this topic:
Background
Especially in the upper cervical region, a high density of muscle spindles provides the proprioceptive input for neck movement.
Various systems are coordinating balance, head neck awareness, movement sense of the cervical spine and head-eye-movement control [1,4]. Where different systems have to do their job, sometimes things may go wrong and “trouble is waiting at the front door”.
Altered afferent input in the cervical region might be a cause of following symptoms: dizziness, unsteadiness, visual disturbances and altered postural stability, cervical proprioception and head eye movement control [4,10]. But also patients, who are not complaining specifically of symptoms like dizziness, unsteadiness or visual disturbance, can suffer from sensorimotor control deficits [4,9].
Disturbance of proprioception may be an important factor in maintenance, recurrence and increase of symptoms [4].
Causes of impaired afferent input can be musculoskeletal disorders such as trauma, swelling, pain, ischemia, fatigue, as well as pathophysiological changes of the peripheral or central nervous system [1,4]. This can lead to decreased sensorimotor control, which can furthermore provoke worse long-term effects [4]. Inhibiting the causes and improving proprioception might be a key for a positive treatment effect [4].
Tests
Therefore is suggested, that each area of sensorimotor control should be investigated in patients with neck pain [4,9]. Various assessments and treatment methods have been developed, to provide a tailored management for neck patients:
- Head-neck awareness: Cervical joint position se
 nse (also known as joint position error) can be assessed by using a laser pointer fixed on a headband. Patients sit in 90cm distance in front of a wall, their head in a natural resting position, the beam of the laser pointer marked on the wall. The task is to move the head actively (with the eyes closed) into rotation, flexion, extension or lateral flexion and back to the starting position. The difference between the starting and end position can be measured in centimetres [4,5,9].
nse (also known as joint position error) can be assessed by using a laser pointer fixed on a headband. Patients sit in 90cm distance in front of a wall, their head in a natural resting position, the beam of the laser pointer marked on the wall. The task is to move the head actively (with the eyes closed) into rotation, flexion, extension or lateral flexion and back to the starting position. The difference between the starting and end position can be measured in centimetres [4,5,9]. - Cervical movement sense: There are several interesting devices to test the accuracy of head/neck movements like “The Fly” or “virtual reality”. These are computer programs, where targets move unpredictably on the screen, and the patient has to follow them by head movements (with a device on the head) [3,4,5,7]. I assume, that not every physiotherapy practic
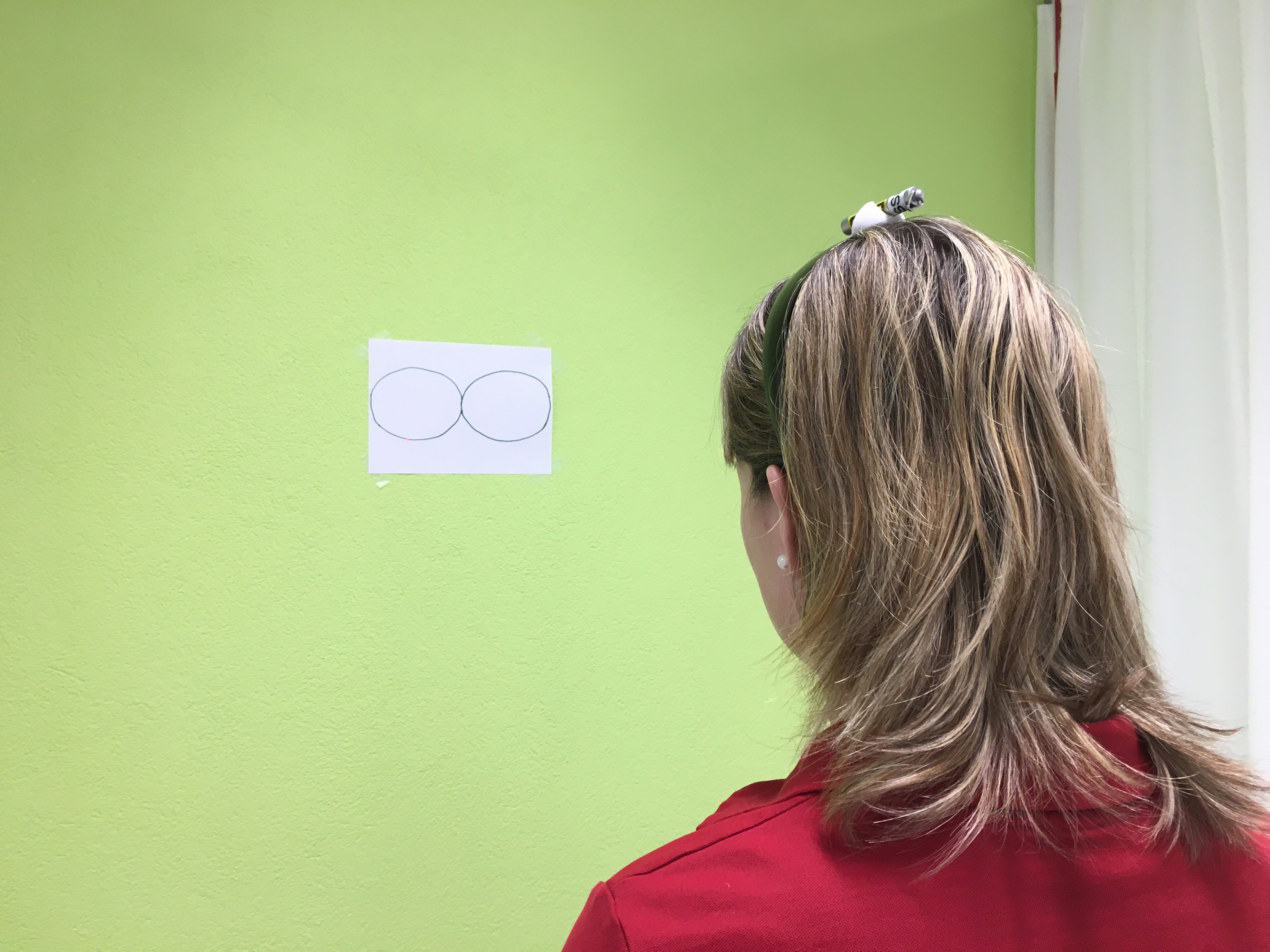
 e has the possibility to own this equipment. So there is – not yet validated – an alternative to use a laser pointer on the head, to trace for example a “figure 8 pattern”, accuracy and smoothness can be evaluated [4]. One disadvantage is, that the factor of unpredictability is not provided; this method might be easier for patients, than the computer programs.
e has the possibility to own this equipment. So there is – not yet validated – an alternative to use a laser pointer on the head, to trace for example a “figure 8 pattern”, accuracy and smoothness can be evaluated [4]. One disadvantage is, that the factor of unpredictability is not provided; this method might be easier for patients, than the computer programs.
- Postural stability: Can be assessed by stopping time in unspecific balance tests like comfort and narrow stance on firm or soft surface, tandem stance or single leg stance with open or closed eyes. In these tests we have to be aware of the age and other diagnosis, which can influence the result. Another possibility to assess balance is the dynamic gait index (DGI) [4].
- Head eye coordination: Different aspects of oculomotor functions have to
[caption id="attachment_6498" align="alignright" width="100"]
 Gaze stability[/caption]
Gaze stability[/caption]be assessed [4,9]. Della casa et al. developed a test battery to assess oculomotor dysfunctions: The patient has to perform different tasks: move his eyes as quickly as possible from the right to the left side and back (saccadic eye movement), while trying not to move the head; move the head, while looking all the time at the same spot (gaze stability); move the eyes to a defined spot and then move the head into the same direction (rotation) separately [2].
- Cervical movement control: This term might look similar to “cervical movement sense”, but there is a difference: “Movement sense” aims to
[caption id="attachment_6499" align="alignright" width="100"]
 Elevation with evasive movement of the cervical spine[/caption]
Elevation with evasive movement of the cervical spine[/caption]assess accuracy and smoothness of neck movement, while the aim of assessing “movement control” is to find evasive movements of the cervical spine during movement tasks. A test battery of 8 different movement tests is suggested by Patroncini et al.. Patients have to perform extension of cervicothoracic junction, upper body forward-backward movement, bilateral shoulder elevation, unilateral shoulder flexion, arm flexion 90° with weight, forward bending in standing, neck flexion in supine position and pro-/retraction, the therapist is checking for evasive movements of the cervical spine [6].



Treatment
For a lasting effect, a multimodal treatment is suggested, which can contain – always chosen according to the clinical reasoning process – the “common” interventions like manual therapy, specific neuromuscular control training, range of motion exercises and soft tissue treatment like trigger point therapy, in combination with a tailored sensorimotor training (may contain head-neck awareness, cervical position sense, cervical movement sense), oculomotor training program (gaze stability, smooth pursuit, head eye coordination) and postural stability [1,4,9].
The sensorimotor deficits found, can be trained by tasks similar to the tests. For example:
- Joint position sense: Can be trained with a laser pointer mounted on the head, performing head movements and relocating back to the neutral position. First with eyes open, then as a progression with eyes closed [1,4,9].
- Cervical movement sense: Tracing patterns mounted on a wall with a laser pointer fixed on the head [1,4].
- Gaze stability: Keep gaze on a dot on the wall, while moving the head passively (by the therapist) or actively [4,9].
- Saccades: Moving the eyes quickly between two dots on a wall [4,9].
- Smooth pursuit: Follow with the eyes a laser light on a wall, while keeping the head in neutral position [4,9].
- Head-eye coordination: Move eyes to a marked point, then move the head in the same direction [4,9].
- Balance: Balance training on firm or unstable surface, with eyes open or closed, various walking tasks [1,4,9].
- Cervical movement control: Incorrect movements in the test can be used as training: for example if bilateral shoulder elevation leads to extension of the cervical spine, the exercise could be shoulder elevation in front of a mirror, with a smaller range of motion, in which the patient can keep the cervical spine stable.
For progression, all sensorimotor tasks can be performed in standing position and on stable or unstable surface [4].
Specific training of proprioception is recommended to perform without provoking pain, swelling or fatigue - as these are the causes for impaired proprioception [1].
In a recent RCT there was no difference found between tailored and random treatment of chronic neck patients [8]. From my point of view the most important point is to stick to the clinical reasoning process. We can try to treat the dysfunctions we found and check with reassessment, if the method chosen is useful for our patient. And if headstand training on a wobble board is indicated for some reason … why not? But please take a picture!
References
[1] Clark, N. C., Röijezon, U., & Treleaven, J. (2015). Proprioception in musculoskeletal rehabilitation. Part 2: Clinical assessment and intervention. Man Ther, 20(3), 378-387. doi:10.1016/j.math.2015.01.009
[2] Della Casa, E., Affolter Helbling, J., Meichtry, A., Luomajoki, H., & Kool, J. (2014). Head-eye movement control tests in patients with chronic neck pain; inter-observer reliability and discriminative validity. BMC Musculoskelet Disord, 15, 16. doi:10.1186/1471-2474-15-16
[3] Kristjansson, E., & Oddsdottir, G. L. (2010). "The Fly": a new clinical assessment and treatment method for deficits of movement control in the cervical spine: reliability and validity. Spine (Phila Pa 1976), 35(23), E1298-1305. doi:10.1097/BRS.0b013e3181e7fc0a
[4] Kristjansson, E., & Treleaven, J. (2009). Sensorimotor function and dizziness in neck pain: implications for assessment and management. J Orthop Sports Phys Ther, 39(5), 364-377. doi:10.2519/jospt.2009.2834
[5] Michiels, S., De Hertogh, W., Truijen, S., November, D., Wuyts, F., & Van de Heyning, P. (2013). The assessment of cervical sensory motor control: a systematic review focusing on measuring methods and their clinimetric characteristics. Gait Posture, 38(1), 1-7. doi:10.1016/j.gaitpost.2012.10.007
[6] Patroncini, M., Hannig, S., Meichtry, A., & Luomajoki, H. (2014). Reliability of movement control tests on the cervical spine. BMC Musculoskelet Disord, 15, 402. doi:10.1186/1471-2474-15-402
[7] Sarig Bahat, H., Chen, X., Reznik, D., Kodesh, E., & Treleaven, J. (2015). Interactive cervical motion kinematics: sensitivity, specificity and clinically significant values for identifying kinematic impairments in patients with chronic neck pain. Man Ther, 20(2), 295-302. doi:10.1016/j.math.2014.10.002
[8] Svedmark, Å., Djupsjöbacka, M., Häger, C., Jull, G., & Björklund, M. (2016). Is tailored treatment superior to non-tailored treatment for pain and disability in women with non-specific neck pain? A randomized controlled trial. BMC Musculoskelet Disord, 17(1), 408. doi:10.1186/s12891-016-1263-9
[9] Treleaven, J. (2008). Sensorimotor disturbances in neck disorders affecting postural stability, head and eye movement control--Part 2: case studies. Man Ther, 13(3), 266-275. doi:10.1016/j.math.2007.11.002
[10] Treleaven, J., Chen, X., & Sarig Bahat, H. (2016). Factors associated with cervical kinematic impairments in patients with neck pain. Man Ther, 22, 109-115. doi:10.1016/j.math.2015.10.015
#neckpain #movementsense #cervicalmovementsense #cervicalspine #nonspecificneckpain #nsnp #cervicalproprioception #proprioception #sensorimotor #sensorimotortraining


Comments