
Should “Education” stand above our “Hands on” Skills?
 Steffen Klittmann
Steffen Klittmann
Currently there is a lot of discussion about "Education" as a treatment option in the physiotherapy profession. There is evidence, that education seems to be more effective than other treatment options (Anneleen et al 2017, Babatunde et al 2017, Dolphens et al 2014, Louw et al 2017, Malfliet et al 2017).
BUT
- What does "Education" mean at all?
- Is this really an important issue or is it overestimated?
The definition of "Education" (Google)
The term "Education" is derived from the Latin word "educare" - i.e. Patients and relatives are to be "led out" from the state of ignorance and inexperience.
A short story about craftsmen and manualtherapists
Like a craftsman, a manual therapist needs his tool kit for his daily work with different examination and treatment techniques. This toolkit should be as comprehensive as possible, in order to have the right tool for the daily problems.
Furthermore, both professions have to know, which tool is suitable for which problem. If the problem is e.g. a dripping faucet, a drilling machine is ineffective. But if you want to drill a hole, then it is the right tool. So, if the manual therapist wants to mobilize a stiff joint, education will not be the tool of choice. But if the therapist wants to explain the patient that he should do a special exercise for further improvement, education will be the right tool.
If the customer or patient has questions about the existing problem, he/she wishes a proper answer and a solution of the problem. Serious craftsmen and manual therapists provide answers to the questions asked.
Some tools are used by craftsmen and manual therapist daily, others perhaps only once a week or even more rarely. Nevertheless, all tools are important for both professionals. If they don´t have the right one at hand, the work can´t be carried out or only suboptimally.
The similarities are part of a problem-solving process = Clinical Reasoning. In this process, many different factors are taken into account and hypotheses are formed, which have to be critically checked for correctness.
How can education be integrated into a manual-therapeutic session?
In manual-therapeutic sessions the content and focus changes over time. In the diagram below, some of content is schematically represented in this process:
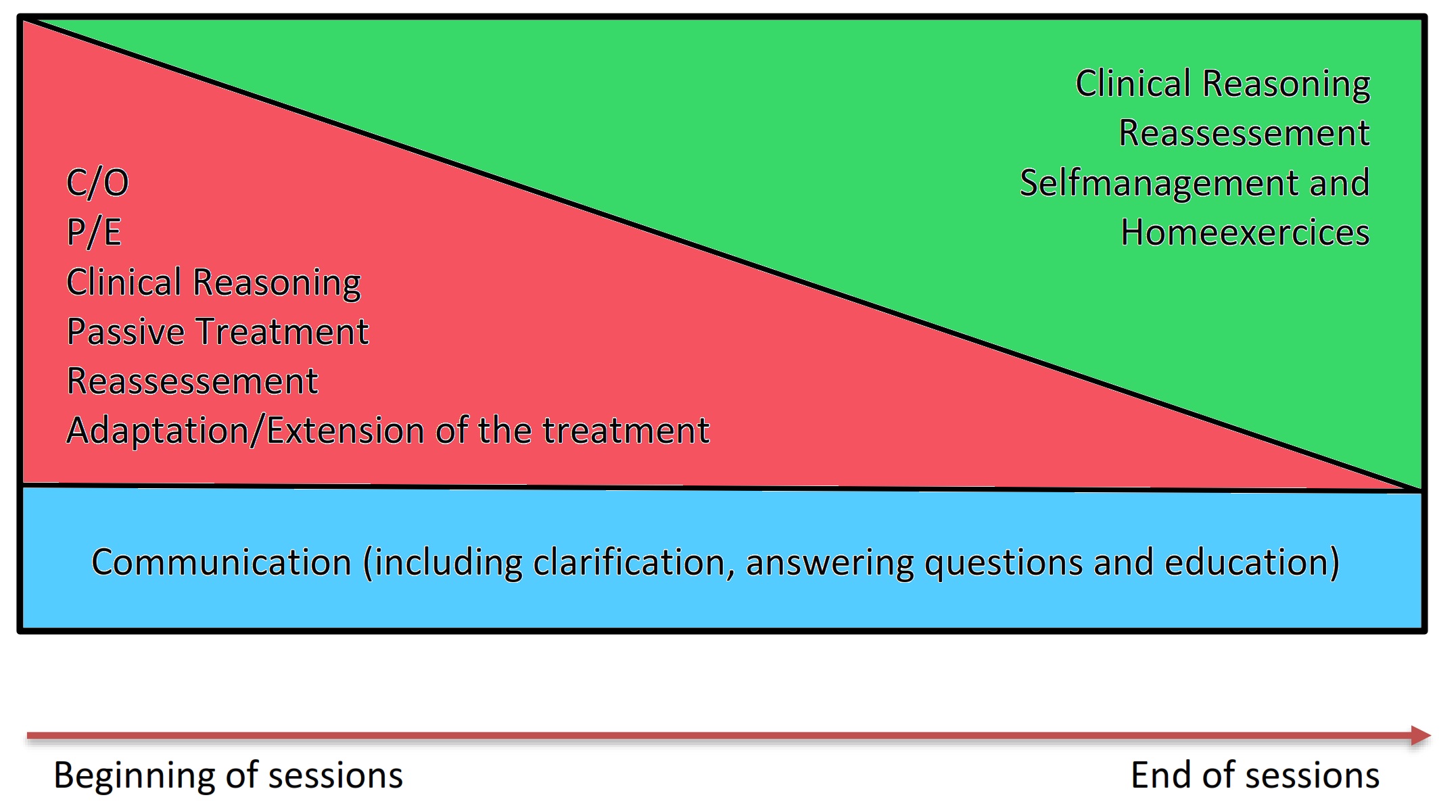
First, the therapist starts with the C/O and P/E. Accompanying this, Clinical Reasoning always takes place. After the treatment, including a reassessement, the therapist reflects his hypotheses and checks them for correctness. If necessary, the additional sessions are adapted to the problem more specifically and extended by additional content. Gradually, the therapist implements self-management strategies and homeexercices for the patient to give him a locus of control.
Should Education stand above our "Hands on" Skills or not?
In this diagram communication is understood as a process, which takes place from the beginning of the sessions to the end of the sessions, parallel to the "Hands on" therapy. Education is part of the communication with the patient.
Each of us is looking forward to get a new tool, which can be used in practice and be tested for the effectiveness. After some time of testing, the tool usually finds a place in the tool box and it is established, that it has become one tool among many. It is useful when the appropriate problem occurs.
So why should it be different with education?
As physio- and manual-therapists, it is our primary task to examine and treat movement dysfunctions. Communication and education are ongoing processes between the patient and the therapist, that already starts with the first contact. Sometimes it needs a little bit of education, sometimes a bit more, in some cases also much. Our task is to find out the necessary amount and content of education in the Clinical Reasoning process and integrate it into the therapy accordingly...
Like the way we do it with any other treatment technique.
5 Take Home Messages:
- Each patient is individual and therefore needs an individual examination and treatment.
- Trust in your Clinical Reasoning: Build and check your hypotheses continuously for correctness.
- Think about your patients´s need for "Education". Especially the content and the necessary amount of it.
- Make sure that your patient understands what you want to explain. For example, let the patient repeat the explained things in his/her own words.
- Answer all questions to your patient as well and correctly as possible. Especially these 4 (Louis Gifford):
- "What´s wrong with me?"
- "How long is it going to take to get better?"
- "Is there anything I can do to help myself?"
- "Is there anything that you can do to help me?"
Education is an exciting topic and everyone is talking about it, but not every patient needs it as a primary therapy!
Cheers,
Steffen
References:
Anneleen, Malfliet; Jeroen, Kregel; Mira, Meeus; u. a. (2017): „Applying contemporary neuroscience in exercise interventions for chronic spinal pain: treatment protocol“. In: Brazilian Journal of Physical Therapy., DOI: 10.1016/j.bjpt.2017.06.019.
Babatunde, Opeyemi O.; Jordan, Joanne L.; Van der Windt, Danielle A.; u. a. (2017): „Effective treatment options for musculoskeletal pain in primary care: A systematic overview of current evidence“. In: PLoS ONE. 12 (6), DOI: 10.1371/journal.pone.0178621.
Dolphens, Mieke; Nijs, Jo; Cagnie, Barbara; u. a. (2014): „Efficacy of a modern neuroscience approach versus usual care evidence-based physiotherapy on pain, disability and brain characteristics in chronic spinal pain patients: protocol of a randomized clinical trial“. In: BMC Musculoskeletal Disorders. 15, S. 149, DOI: 10.1186/1471-2474-15-149.
Louw, Adriaan; Nijs, Jo; Puentedura, Emilio J. (2017): „A clinical perspective on a pain neuroscience education approach to manual therapy“. In: Journal of Manual & Manipulative Therapy. 25 (3), S. 160–168, DOI: 10.1080/10669817.2017.1323699.
Malfliet, Anneleen; Oosterwijck, Jessica Van; Meeus, Mira; u. a. (2017): „Kinesiophobia and maladaptive coping strategies prevent improvements in pain catastrophizing following pain neuroscience education in fibromyalgia/chronic fatigue syndrome: An explorative study“. In: Physiotherapy Theory and Practice. 0 (0), S. 1–8, DOI: 10.1080/09593985.2017.1331481.
#education #manualskills #explanation #manualtherapy #handson


Comments