Screening for red flags – possible after week 1
 Jürg Hauswirth
Jürg Hauswirth
Recognizing red flags or precaution with a screening process for further treatment is possible already after the first course week in the Maitland Concept!
One of the most important things in teaching the Maitland Concept is that the students will be able to transfer what they learned to the clinical ground in their daily practice.
At the end of the first course week I always tell my participants, that they now are the specialists of the lumbar spine and “experts” in detecting important precautions or contraindications. One key aspect of the physical examination is an exact neurological examination with testing the sensitivity, muscles innervation and reflexes.
And so in Warsaw, at the very start of the second course week, one participant - Tomasz Waraksa-came to me and told a story of one of his patient. In my opinion this is a good story to share with all participants, to highlight the importance of conducting a thorough neurological examination with your patients, when indicated.
Here it is:
INTRO
26 years old patient came to the clinic with tingling sensation along his left lower limb. Symptoms occured more than six months earlier without any clear onset. Patient was reffered to the physiotherapist by the orthopaedic specialist with diagnosis of the discopathy on L5/S1 (?) level.
C/O
1. Main problem.
Patient’s main problem was a sensation of tingling along the lateral surface of his left lower limb (from hip down to the ankle). Patient also reported, that sometimes he wouldn’t feel his left foot eg. during changing gears on a motorbike. He also reported about problems with strength and precision in his left hand. Symptoms in the foot and hand weren’t constant, but very often appear together.
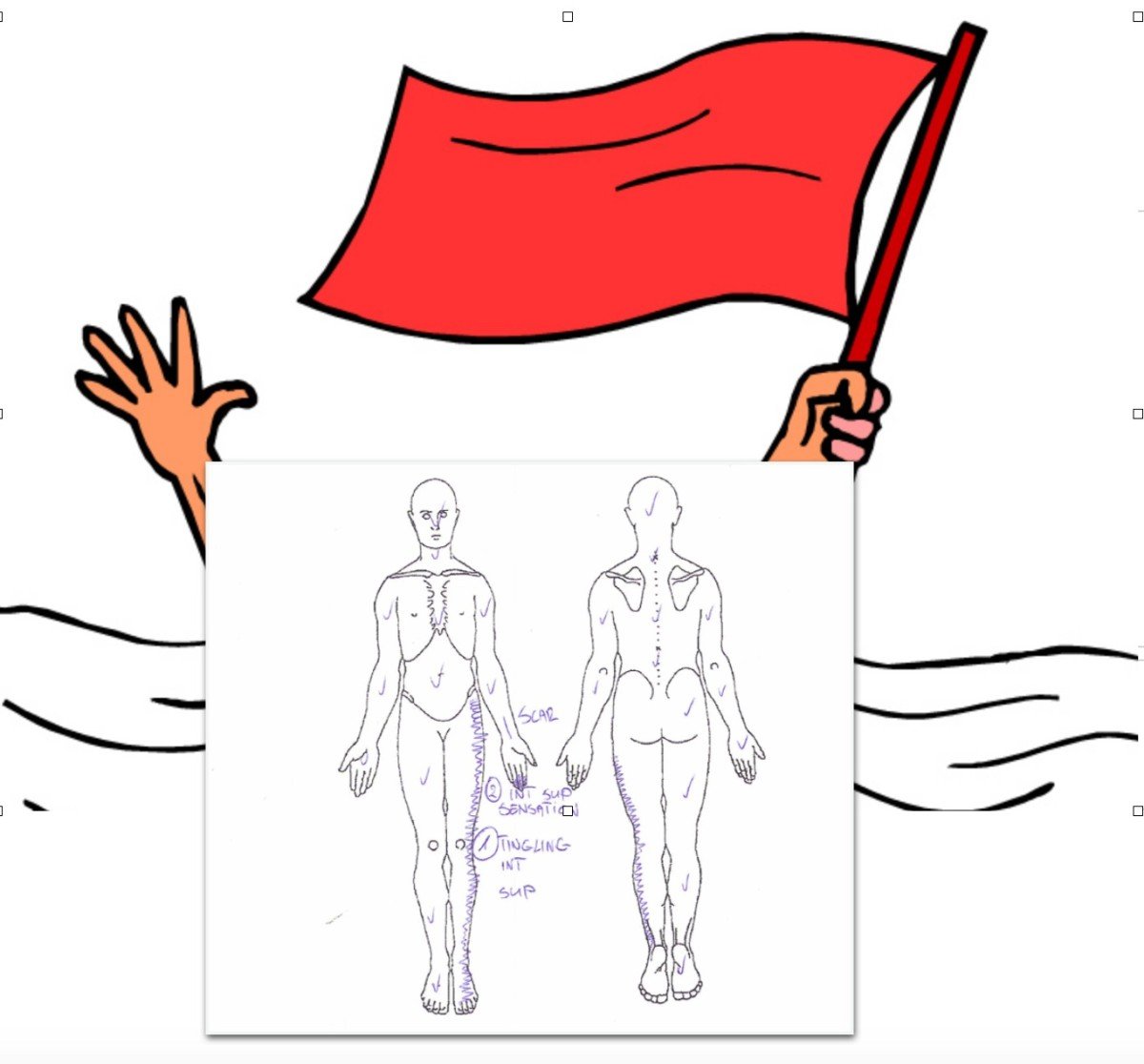
2. Body chart.
Pins and needles - ? (more like tingling)
Unsure gait - √
Vision - √
Dizziness - √
Urination/Defecation – needs to spend more time for urination than usually.
3. 24h.
No night problems.
In the morning symptoms increased, but after several steps usually disappeared.
Sitting with bend legs increased symptoms (extension decreased symptoms).
4. Hx.
First symptoms (tingling L thigh and problems with L hand ) occured during autumn 2017. They weren’t constant, but episodic.
5. Special questions.
01.08.2015 – car accident – L thigh fracture (scar on the L thigh lateral surface); without any CNS damage.
Few months earlier during working patient cut his upper limb along the L hand and wrist – suspicion of median nerve damage.
Patient had been waiting for MRI (lumbar spine) and EMG (left hand).
P/E
1. Present Pain.
Feeling of tingling of the left lower limb (hipankle).
2. Inspection.
Pelvis correction ↓anterior tilt √
Weight bearing correction to R √
L-S shift to R √
3. Active movements
Lx FFD (touch the floor) √
Lx E √
Lx ROT L √
Lx ROT R √
Lx LAT FL L √
Lx LAT FL R √
4. Neurological examination
Superficial sensitivity – dysesthesia in all dermatomes from the L costal arch to the L ankle (patient didn’t feel that he had been touched). Patient reported that on the R lower limb he felt 100% and on the L 30%.
Deep sensitivity (mirror test) – failed in the L foot.
Babinski reflex – present on the L; R √.
Reflexes (assessed on the 2nd appointment)
L R
Biceps ++ ++
Triceps ++ ++
Brachioradialis* ++ ++
Quadriceps ++ ++
Achilles ++ ++
5.
*Jacobson Reflex present during Brachioradialis reflex
CONCLUSION:
PT referred patient to the neurologist. During hospitalization further medical screening was done:
- Brain MRI
Changes in the right parietal lobe (cortical and subcortical). Right lateral ventricle was enlarged.
- Lumbar spine MRI
Herniated/disc bulging to the central and left side on the L5-S1 level.
- Angio CT
R ICA narrowed to 3 mm (L ICA 6 mm).
Note: There is no clear diagnosis yet. Specialists suspects thrombophilia/rheumatoid origins/Moyamoya disease.
Additional comment:
Even though a lot of cases of spinal pain are described as non-specific and benign it is recommended by most guidelines that screening for serious pathologies are essential steps of your examination process. To assist in this process, red flags screening is recommended for identifying patient with serious medical condition. Referring every patient with a single red flag for further investigation is not practical and would lead to increases costs. Therefore, the decision to refer is much more complex and requires that subjective and objective physical findings are integrated into clinical reasoning process.
“Hence the importance of a proper C/O and P/E - connecting facts, thinking in hypothesis categories, and not only relying on the medical diagnosis.
It takes courage to tell the patient in the eye: “Well, maybe it would be better if another specialist assessed you as well.” But this is no sign of weakness! In fact, that’s the only fair thing we can do for such patient.
This case from a participant of a Maitland course highlights the essential role that all clinicians play in the role of screening for serious pathologies. The interpretation of these clusters of subjective and physical examination findings may lead to refer for further medical investigation.
Special thanks to Tomasz Waraksa/ participant of Level1 in Warsaw
Jürg


Comments