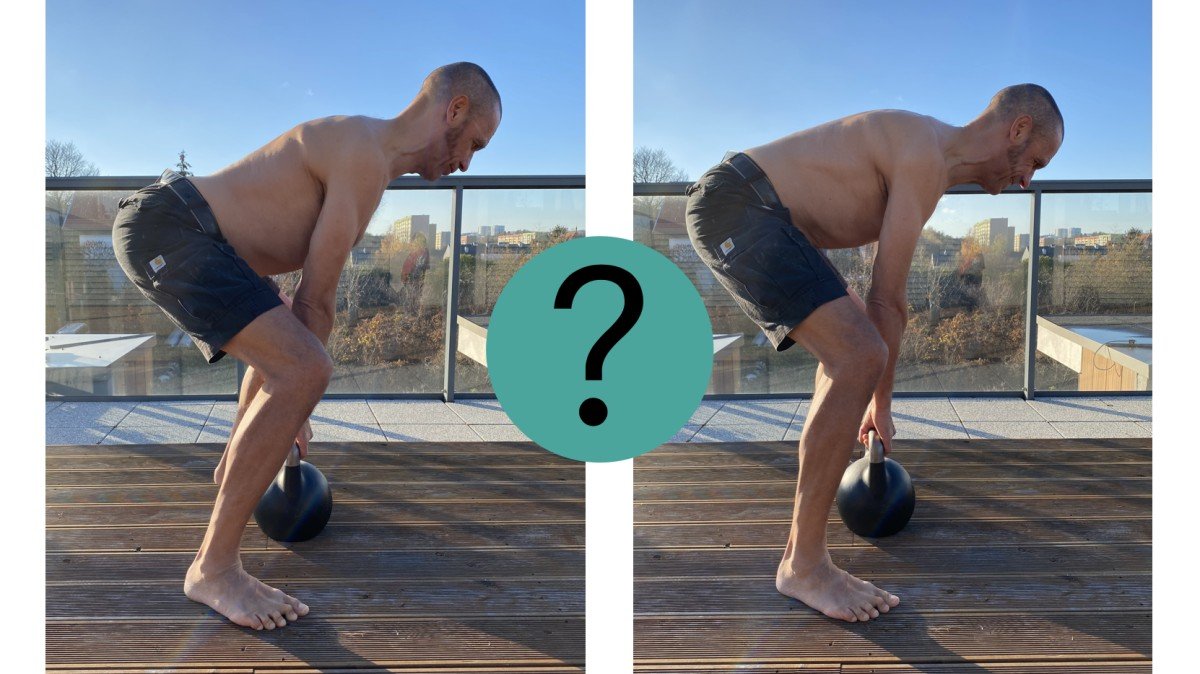
“How should I lift this thing from the floor?” Straight or flexed back – what do YOU think?
 Daria Frozyna
Daria Frozyna
Lifting is considered as a common risk factor for development and exacerbation of low back pain (LBP) [10,11,32].
It is taught in nearly every workplace health and safety course around the world that you need to keep your back straight when you lift or you’ll hurt it. Yet ironically, it seems to be a bit of a dogma that has lasted through the ages, because there is almost no evidence it is true. Moreover, there is also no evidence that lifting with a flexed / round back increases the risk of back pain.
What do we, physical therapists (as movement experts and health-care providers), think about this issue? How do we educate our patients and how much our approach reflects the current state of knowledge?
Fear of bending
The conventional wisdom carries a strong and long-held belief, that the back is easily injured, its healing process is long and lifting with a flexed lumbar spine is generally harmful and has a causative role in lifting- related low back pain (LBP).
When bending down people are afraid to “slip or blow their disc”. This notion has extended out to the degree where some people will fear even the concept of picking up something as light as a feather without a perfectly straight back.
In patients with LBP, pain-related fear has been shown to be strongly associated with reduced lumbar flexion range of motion during lifting [6]. It means, that fear alone can increase protective behaviours, including avoidance of daily activities. However, despite short-term beneficial effects for tissue health, maintaining a protective trunk movement strategy (i.e. not flexing the spine) may also pose a risk for persistent LBP. Rigid motor behaviour and increased muscle co-contraction, lead to increased mechanical loading on spinal tissues, and in long term to pronociceptive consequences, linked to deterioration of (para)spinal tissues and decreased movement variability [12].
Interestingly, this fear does not only exist in people suffering from LBP, but also in asymptomatic adults without a history of chronic pain [18]. That means, that pain-free population holds a pre-existing belief about lifting, that the back is in danger when rounded [5].
The “dangerous bending” and physiotherapists
Flexed back danger beliefs can be unhealthy, yet they are often communicated by healthcare professionals. Over 75% of physical therapists hold this belief (!), which can strongly influence their advice to patients, potentially reinforcing unhelpful protective and/or avoidance behaviours, while attitudes and beliefs of patients are important in the recovery from an episode of back pain [7,26].
The beliefs of physiotherapists may be explained by the type of training they got, still these days based largely on a pathoanatomical and biomechanical paradigm and deficits in continuing professional education [26]. Therefore there is a great need of promoting new education campaigns, to emphasise a ‘trust your back’ message rather than a ‘protect your back’ message while encouraging activity [8,27].
When did it all start?
Back in the 80’s and 90’s the scientific rationale emerged to recommend straight and not round back lifting, since the latter was thought to be associated with increased risk of herniated lumbar disc [23,24,25]. Back schools, including the “safe lifting technique”, were introduced in occupational settings, and soon after these recommendations extended into daily functioning.
After many years the effectiveness of manual handling training programs has been questioned [9,14,15,20,31] concluding, that such training activities either show no significant results, or at best, offer marginal benefits in preventing injuries.
Why? Often provision of knowledge does not necessarily mean application of knowledge, and knowledge acquired may not be optimal or not applicable to the specific workplaces or exposures involved [3,29]. It is also quite unlikely, that an optimal lifting technique exists for all individuals under all conditions [13]. Besides, is it really only the lifting technique?
What do we know now?
Spine motion during lifting is constrained not only by biomechanics, but also by a variety of interacting personal, task, and environmental factors [3].
LBP in turn is a multifactorial condition, which is rather not a single disease state, but a symptom, whose presence does not reveal much about the underlying factors that cause it. There is no consensus regarding causality of physical exposure (e.g. amount of lumbar flexion) to LBP.
- Spinal flexion is highly functional; it’s unavoidable (at least in 50-70% of its maximal range).
- There are studies, mainly cadaveric, which supports an argument, that lumbar flexion does pose a possible mechanism to injury. In cadaveric studies, however, the element of adaptability of human body structures is omitted. In fact, repeated flexion and repeated loading may be a good thing for the structures of the spine (discs, ligaments), as these structures can strengthen and heal over time. Moreover, in in-vitro studies discs are exposed to dozens of thousands of consecutive cycles of flexion, without moments of rest, therefore - however good and informative - these studies do not reflect a real life situation (have you met anyone, who would dare to perform eg. 86.400 of sit-ups in a row, like in some of the in-vitro studies :)
- Recent biomechanical in-vivo studies in pain-free populations do not support a substantial difference in the increase of spinal loads (disc pressure, compression or shear strain) between flexed versus straight back lifting. Greater lumbar spine flexion during lifting was not a risk factor for LBP onset, persistence or recurrence [28,33].
- There is very limited to no evidence that spinal flexion is an independent risk factor for LBP, it is therefore more a combination of spine kinematics and kinetic force (load). Various aspects associated with flexion have to be taken into account – number of repetitions/cycles, duration of stretch, compression rate.
- In lifting heavy objects not only the lifting technique is of importance, but also weight of the lifting object, lifting speed, size of the weight, load-splitting, weight location, spinal posture, mental processing. [2]
- With more flexion while lifting loads there is more stress on passive tissues (ligaments, discs, fascia) and less on the muscle.
- Repetitive and prolonged lumbar flexion, can lead to cumulative creep in passive ligamentous and musculature systems, decreases in disc stiffness, and flexion relaxation phenomenon, thereby deteriorating the spinal stability. On the other hand, the overall segmental compressive/shear forces markedly increased in lordotic postures. [16]
- In lordotic postures muscles are working more and they are more metabolically demanding.
- Lifting with a flexed spine significantly increases lumbar extensor moment and enhances neuromuscular efficiency, therefore overall strength and metabolic efficiency. [21,22]
- Factors such as repetitive lifting when fatigued, or having poorer mental and physical health, might also be more important than solely the way of lifting.
- There is no research showing that a flexed spine is stronger when it comes to injury or pain.
Is flexion possible to avoid at all?
No! Spinal flexion is largely functional, unavoidable, irrespective of the setting: we cannot avoid it in sports, in rehabilitation process, in daily life. Even if we really try to.
Pertaining to lifting, if we are looking at it from a perspective of low load / rate activities (e.g. picking up a pencil from the floor), the evidence clearly suggest that it does not matter whether it is performed with a “flexed” or “neutral” spine.
When discussing various sports, where the loads or rates of flexion are higher, the recommendation will likely shift back and forth, depending on the discipline. Sporting demands require inherently different postures and capacities. However, in many of them, like: cycling, skiing, rowing, throwing, golf, wrestling, flexion (often repeated) is an inseparable element and a necessity. Even those sports which are flexion biased, do not have greater degrees of low back pain versus those in neutral [30].
Nevertheless, majority of training programs for athletic development, physique enhancement, or rehabilitation, would still follow the trend of avoiding exercises clearly involving flexion. But yet the proposed alternatives may not be anyhow better when we compare the loads on the spine. While normal range of maximal lumbar flexion is around 60º [17,19], simple squatting, when trying to be in so called “neutral”, can see even 40º (which is 65% of maximal flexion, in a theoretically “ideal lifting technique” as understood by most people) [4,17]. Or a kettlebell swing involves on average 26º of lumbar flexion [35]. When bending in a lordotic position, there is around 22º of flexion. In the studies, despite being verbally instructed to prevent rounding of the lower back, all participants flexed their spine when lifting and lowering [3].
As we get into lifting heavy objects, the discussion takes on even more colour. When looking at individuals performing maximal lifting events, it is not uncommon to see a change from neutral to flexion, eg. in deadlifts. Even though power lifters have been shown to lift in moderate to high degrees of lumbar flexion [1], the lifting advice here will still likely shift more in favour of the “neutral” plus the hip hinge. The experts [34] highlight, that this approach aims NOT to reduce risk of any injury, but is performance dependent. Getting into a good hip hinge allows to maximise the hamstrings contribution to the lift and is also the optimal position to produce power from, therefore it provides a mechanical advantage to lifting heavy weights.
And even though some research suggests that flexion may not be worse than neutral, there is no research showing it is safer. High load activities are examples where biomechanics are important, because often these loads may exceed the structural strength of the tissue.
Is it then only high loads, where we should care?
While we have a scientific permission to care very little about spinal flexion under many conditions, there are still other conditions, under which it is more reasonable to try and avoid excessive rounding of the back. When for example?
Surely, temporarily when the back is sensitised. With acute LBP, the brain may perceive lumbar flexion as a "threatening" motion, so it may be beneficial to avoid it for a little and train other movement patterns. However, once the threat decreases, it is ESSENTIAL to slowly re-integrate the movement of lumbar flexion. Trying to keep the back as lordotic as possible is very energy demanding and an inefficient posture to use.
Minimising spinal flexion is also a solution for cases, where highly repetitive flexion is shown to be associated with pain (some people are simply not able to adapt; some demands are simply too big to adapt to).
Additionally, as mentioned before, certain types of training/performance are more efficient when lumbar flexion is not being taken to its extremes.
So, how to lift things?
The evidence about the most optimal lifting technique is not quite as clear as many people believe, but perhaps it’s not so much the matter of HOW you lift, but rather if you are PREPARED to lift things. The spine can cope with huge loads, as long as they are introduced in a progressive way, over time, allowing the body to adapt. Therefore gradual building tolerance to lifting is of a big importance. And this in turn, is a very positive information for us, physical therapists! So get rid of all you negative beliefs about the spine, stop feeding your patients with fear-avoidance behaviours and encourage them to have more trust in their own body! :)
REFFERENCES
[1] Aasa U, Bengtsson V, Berglund L, Öhberg F. Variability of lumbar spinal alignment among power-and weightlifters during the deadlift and barbell back squat. Sports Biomech 2019; 13: 1-17.
[2] Amin DB, Tavakoli J, Freeman BJC. Mechanisms of Failure Following Simulated Repetitive Lifting: A Clinically Relevant Biomechanical Cadaveric Study. Spine (Phila Pa 1976) 2020; 45(6):357-367.
[3] Beach TAC, Stankovic T, Carnegie DR. Using verbal instructions to influence lifting mechanics – Does the directive “lift with your legs, not your back” attenuate spinal flexion? J of Electromyography and Kinesiology 38 (2018) 1–6.
[4] Bengtsson V, Berglund L, Aasa U. Narrative review of injuries in powerlifting with special reference to their association to the squat, bench press and deadlift. BMJ Open Sport & Exercise Medicine 2018; 4(1).
[5] Caneiro JP, O’Sullivan P, Lipp OV. Evaluation of implicit associations between back posture and safety of bending and lifting in people without pain. Scand J Pain 2018; 18:719–28.
[6] Caneiro JP, O’Sullivan P, Smith A. Implicit evaluations and physiological threat responses in people with persistent low back pain and fear of bending. Scand J Pain 2017; 17:355–66.
[7] Caneiro JP, O’Sullivan P, Smith A. Physiotherapists implicitly evaluate bending and lifting with a round back as dangerous, Musculoskelet. Sci. Pract. 2019; 39: 107–114.
[8] Christe G, Darlow B, Pichonnaz C. Changes in physiotherapy students’ beliefs and attitudes about low back pain through pre-registration training. Archives of Physiotherapy 2021; 11:13.
[9] Clemes SA, Haslam CO, Haslam RA. What constitutes effective manual handling training? A systematic review. Occup. Med. 2009; 60(2):101–107.
[10] Coenen P, Gouttebarge V, van der Burght AS. The effect of lifting during work on low back pain: a health impact assessment based on a meta- analysis. Occup Environ Med. 2014; 71(12):871-877.
[11] Cole MH, Grimshaw PN. Low back pain and lifting: a review of epidemiology and aetiology. Work. 2003; 21(2): 173-184.
[12] Cote JN, Hoeger Bement MK. Update on the relation between pain and movement: consequences for clinical practice. Clin J Pain 2010; 26:754–62.
[13] Denis D, Gonella M, Comeau M, Lauzier M. Questioning the value of manual material handling training: a scoping and critical literature review, Appl. Ergon. 2020; 89.
[14] Haslam C, Clemes S, McDermott H. Manual Handling Training – Investigation of Current Practices and Development of Guidelines. HSE, 2007. Loughborough, p. RR583.
[15] Hogan DAM, Greiner BA, O’Sullivan L. The effect of manual handling training on achieving training transfer, employee’s behaviour change and subsequent reduction of work-related musculoskeletal disorders: a systematic review. Ergonomics 2014; 57(1), 93–107.
[16] Khoddam-Khorasani P, Arjmand N, Shirazi-Adl A. Effect of changes in the lumbar posture in lifting on trunk muscle and spinal loads: a combined in vivo, musculoskeletal, and finite element model study, J. Biomech. 2020; 104.
[17] Kingma I, Faber GS, van Dieen JH. How to lift a box that is too large to fit between the knees. Ergonomics 2010; 53(10):1228-38.
[18] Knechtle D, Schmid S, Suter M. Fear-avoidance beliefs are associated with reduced lumbar spine flexion during object lifting in pain- free adults. Pain 2021; 162(6): 1621–1631.
[19] Magee D, Manske R. Orthopedic Physical Assessment. 7th Edition. Saunders 2018.
[20] Martimo KP, Verbeek J, Karppinen J. Manual Material Handling Advice and Assistive Devices for Preventing and Treating Back Pain in Workers. 2007; John Wiley & Sons (Review).
[21] Mawston GA, Boocock MG. Lumbar posture biomechanics and its influence on the functional anatomy of the erector spinae and multifidus, Phys. Ther. Rev. 2015; 20 (3):178–186.
[22] Mawston G, Holder L, O’Sullivan P, Boocock M. Flexed lumbar spine postures are associated with greater strength and efficiency than lordotic postures during a maximal lift in pain-free individuals. Gait & Posture 2021; 86: 245–250.
[23] Mundt DJ, Kelsey JL, Golden AL. An epidemiologic study of non-occupational lifting as a risk factor for herniated lumbar intervertebral disc. Spine 1993, 18 (5): 595-602
[24] Nachemson A, Elfstrom G. Intravital dynamic pressure measurements in lumbar discs. A study of common movements, maneuvers and exercises. Scand J Rehabil Med Suppl 1970; 1:1–40.
[25] Nachemson A. The load on lumbar disks in different positions of the body. Clin Orthop Relat Res 1966; 45:107–22.
[26] Nolan D, O’Sullivan K, Stephenson J. What do physiotherapists and manual handling advisors consider the safest lifting posture, and do back beliefs influence their choice? Musculoskelet Sci Pract. 2017; 33:35–40.
[27] Nolan D, O’Sullivan K, Stephenson J. How do manual handling advisors and physiotherapists construct their back beliefs, and do safe lifting posture beliefs influence them? Musculoskelet Sci Pract. 2019; 39: 101-106.
[28] Saraceni N, Kent P, Ng L. To flex or not to flex? Is there a relationship between lumbar spine flexion during lifting and low back pain? A systematic review with meta-analysis, J. Orthop. Sports Phys. Ther. 2019; 1–50.
[29] Sowah D, Boyko R, Antle D. Occupational interventions for the prevention of back pain: Overview of systematic reviews. J of Safety Research 2018; 66: 39–59.
[30] Stange Foss I, Holme I, Bahr R. The prevalence of low back pain among former elite cross-country skiers, rowers, orienteerers, and nonathletes: a 10-year cohort study. Am J Sports Med. 2012; 40(11): 2610-6.
[31] Verbeek JH, Martimo KP, Karppinen J. Manual Material Handling Advice and Assistive Devices for Preventing and Treating Back Pain in Workers. 2011; John Wiley & Sons (Review).
[32] Verbeek JH, Martimo KP, Kuijer PP, Karppinen J, Viikari-Juntura E, Takala EP. Proper manual handling techniques to prevent low back pain, a Cochrane systematic review. Work. 2012; 41 Suppl 1:2299-2301.
[33] Dreischarf M, Rohlmann A, Graichen F. In vivo loads on a vertebral body replacement during different lifting techniques. J Biomech. 2016; 49(6): 890-895.
[34] https://barbellrehab.com/stop-fearing-spinal-flexion/
[35] McGill S, Marshall LW. Kettlebell swing, snatch, and bottoms-up carry: back and hip muscle activation, motion, and low back loads. J Strength Cond Res. 2012; 26(1):16-27.

Comments