
"Modern Manual Therapy as Manipulation of the Brain “ A Holistic Approach to Treating Neck Pain
 Jürg Hauswirth
Jürg Hauswirth
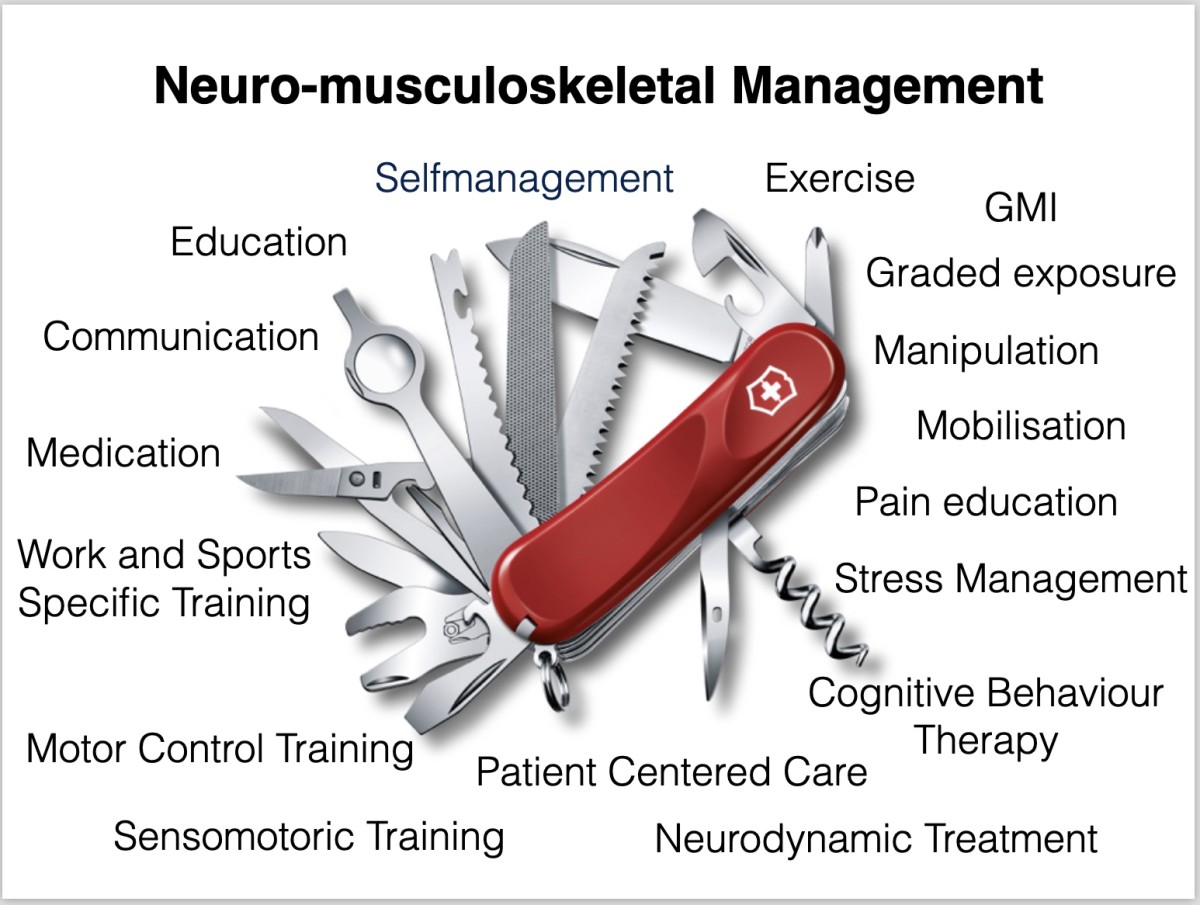
Over the last 20-30 years, pain research has made significant progress, meaning that the way we treat neck pain has evolved considerably. When a patient with neck pain and restricted movement enters my practice for the first time, as a physiotherapist with specialized manual therapy training,
I am faced with a wide range of options to address his problem. (see illustration)
These advances are the result of a fascinating understanding of pain, particularly persistent pain that can lead to changes in the central nervous system. This allows the application of new, evidence-based approaches, such as Graded Motor Imagery (GMI) or pain-based education, to effectively treat nociplastic pain problems (1,2,3).
Nociplastic pain mechanisms refer to the perception of pain that is not due to specific tissue damage or inflammation. Instead, this pain arises due to changes in the nerves and central nervous system. These changes can lead to the amplification or excessive perception of pain signals, even if there is no obvious physical cause for the pain. Nociplastic pain with central sensitization is often chronic and complex, typically requiring comprehensive multimodal medical care and treatment.(4)
The question, however, is whether we are moving too far away from a patient-centered approach with this nociplastic approach. It seems that many physiotherapists are less likely to use manual techniques, possibly due to concerns about promoting dependency behaviors in patients with persistent pain. So, what to do when you have a patient sitting in front of you with neck pain? Of course, it all starts with a comprehensive assessment, identifying the main problem. Are there any possible contraindications, indications of red flags/ yellow flags or precautionary situations? The choice of therapeutic approaches should be based on a well-founded hypothesis of the prevailing pain mechanisms.
Manual therapy, which has been used for centuries, remains a valuable technique. Previous studies have shown that it can have both local and global effects on the body (5). In addition to local effects, manual therapy can also have global influences on hormones and neurotransmitters that can affect central pain processes.

Our understanding of more complex supraspinal mechanisms is evolving. Manual therapy can reduce temporal summation and nociceptive reflexes, affecting nociceptive input to the central nervous system (5). Furthermore, changes in activity in the insular cortex were found in individuals undergoing manual therapy interventions, correlating with a reduction in the subjective experience of pain. Interestingly, these effects were independent of the specific manual technique, whether it was manipulation, mobilization or soft tissue mobilization (6, 7).
Applying these insights in clinical practice requires a differentiated approach. Recognizing the predominant pain mechanisms and considering the patient's expectations are of crucial importance. A multimodal approach combining manual therapy, pain education, exercises and other techniques allows for comprehensive and patient-centered care. (see photos)
In line with this, the following perspective from Chad Cook, American physiotherapist and researcher, is fitting: "Manual therapy should be based on the same philosophical considerations as the use of pain medication. Analgesics provide short-term pain relief that allows the patient to perform activities of daily living or exercise. MT can achieve the same and is unlikely to be beneficial as a stand-alone intervention. At best, MT is part of a multimodal care approach (value based care) (8)
Finally, I would like to draw your attention to the upcoming
IFOMPT Congress in Basel from July 4-6, 2024, which offers a great opportunity to delve into the international discourse on pain research and manual therapy, exploring current developments in this field.
https://www.ifomptbasel2024.org/frontend/index.php
Author, photos and illustration: Jürg Hauswirth
Literature
1. Winkelstein, B. A. (2004). Mechanisms of central sensitization, neuroimmunology & injury biomechanics in persistent pain: implications for musculoskeletal disorders. Journal of Electromyography and Kinesiology, 14(1), 87-93. doi: 10.1016/j.jelekin.2003.09.017
2. Latremoliere, A., & Woolf, C. J. (2009). Central sensitization: a generator of pain hypersensitivity by central neural plasticity. The Journal of Pain, 10(9), 895-926. doi: 10.1016/j.jpain.2009.06.012
3. Thomas Cheng, H. (2010). Spinal cord mechanisms of chronic pain and clinical implications. Current Pain and Headache Reports, 14(3), 213-220. doi: 10.1007/s11916-010-0111-0
4. Kosek, Evaa,b,*; Clauw, Danielc; Nijs, Jod,e,f; Baron, Ralfg; Gilron, Ianh; Harris, Richard E.c; Mico, Juan-Antonioi; Rice, Andrew S.C.j; Sterling, Michelek. Chronic nociplastic pain affecting the musculoskeletal system: clinical criteria and grading system. PAIN 162(11):p 2629-2634, November 2021. | DOI: 10.1097/j.pain.0000000000002324
5. Bishop, M. D., Torres-Cueco, R., Gay, C. W., Lluch-Girbés, E., Beneciuk, J. M., & Bialosky, J. E. (2015). What effect can manual therapy have on a patient’s pain experience? Pain Management, 5(6), 455-464. doi: 10.2217/pmt.15.39
6. Bialosky, J. E., Beneciuk, J. M., Bishop, M. D., Coronado, R. A., Penza, C. W., Simon, C. B., & George, S. Z. (2018). Unraveling the Mechanisms of Manual Therapy: Modeling an Approach. Journal of Orthopaedic & Sports Physical Therapy, 48(1), 8-18. doi: 10.2519/jospt.2018.7476
7. Bialosky, J. E., Bishop, M. D., Price, D. D., Robinson, M. E., & George, S. Z. (2009). The mechanisms of manual therapy in the treatment of musculoskeletal pain: a comprehensive model. Manual Therapy, 14(5), 531-538. doi: 10.1016/j.math.2008.09.001
8. Cook, C. E. (2021). Dämonisierung der Manuellen. Thieme MSK – Muskuloskelettale Physiotherapie, 25(03), 125-131. doi: 10.1055/a-1499-5262
Comments
 Thomas Horre
Thomas Horre Thomas
- {{ error[0] }}
