Sintomi di stress post-traumatico e dolore cronico
" Je ne sais pas ce que le passé nous réserve." Françoise Sagan, Les faux-fuyants, 1991
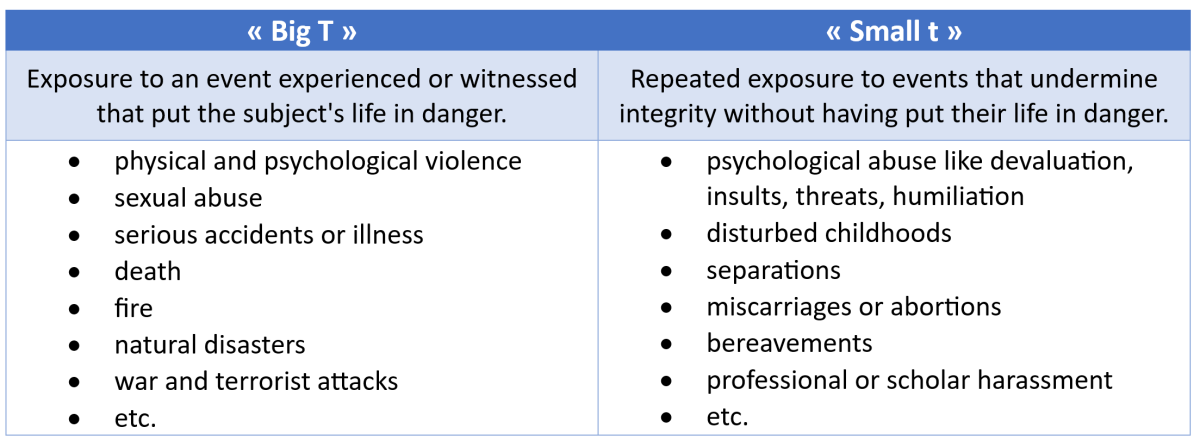
Ci sono traumi con la T minuscola e traumi con la T grande. Il grande è evidente, violento. Il piccolo può passare inosservato. Nessuno di loro va sottovalutato e una piccola T può nascondere una grande T.
Disagio emotivoI disturbi dovuti a esperienze traumatiche possono interferire con il comportamento umano. I fisioterapisti devono essere consapevoli che i sintomi fisici possono essere un tipo di espressione del disturbo post-traumatico da stress (PTSD), "un disturbo psichiatrico che può verificarsi in persone che hanno vissuto o assistito a un evento traumatico, a una serie di eventi o a un insieme di circostanze", come definito dall'American Psychiatric Association.
C'è un'alta prevalenza di sintomi da stress post-traumatico (PTSS) nei pazienti che soffrono di dolore cronico diffuso, con più di 20% di loro che riportano livelli più alti di intensità del dolore, fastidio del dolore, disabilità, disagio psicologico, livelli più bassi di auto-efficacia, livelli più alti di catastrofizzazione del dolore, ingiustizia percepita, affaticamento e difficoltà di sonno. (Linnemørken et al., 2020). Sono state osservate correlazioni positive tra la gravità del trauma e la diffusione del dolore, il dolore massimo, la compromissione del sonno, il Pain Disability Index, lo stress, l'ansia, la depressione e la somatizzazione. (Manuel et al., 2023).
Si raccomanda di sottoporre a screening i pazienti affetti da dolore cronico per il PTSD, poiché sono state dimostrate associazioni con la sensibilizzazione centrale e si è ipotizzata una relazione causale. (McKernan et al., 2019). I clinici che si occupano di pazienti che soffrono di dolore cronico devono tenerne conto e indagare sia la storia attuale che quella passata, prestando maggiore attenzione al PTSS. L'uso della PCL-5 è raccomandato in contesti non psichiatrici. (Merians et al., 2023).
Le terapie cognitivo-comportamentali sono trattamenti di prima linea. Possono essere proposte insieme a quelle farmacologiche. Risorse informative per i pazienti sono disponibili, tra l'altro, presso l'American Psychiatric Association (www.psychiatry.org).
Linnemørken, L. T. B., Granan, L.-P., & Reme, S. E. (2020). Prevalenza di sintomi di stress post-traumatico e caratteristiche associate tra i pazienti con condizioni di dolore cronico in una clinica del dolore ambulatoriale di un ospedale universitario norvegese. Frontiere della psicologia, 11, 749. https://doi.org/10.3389/fpsyg.2020.00749
Manuel, J., Rudolph, L., Beissner, F., Neubert, T.-A., Dusch, M., & Karst, M. (2023). Eventi traumatici, disturbo da stress post-traumatico e sensibilizzazione centrale nei pazienti affetti da dolore cronico di un ambulatorio universitario tedesco. Medicina psicosomatica, 85(4), 351-357. https://doi.org/10.1097/PSY.0000000000001181
McKernan, L. C., Johnson, B. N., Crofford, L. J., Lumley, M. A., Bruehl, S., & Cheavens, J. S. (2019). I sintomi di stress post-traumatico mediano gli effetti dell'esposizione al trauma sugli indicatori clinici della sensibilizzazione centrale nei pazienti con dolore cronico. La rivista clinica del dolore, 35(5), 385-393. https://doi.org/10.1097/AJP.0000000000000689
Merians, A. N., Spiller, T., Harpaz-Rotem, I., Krystal, J. H., & Pietrzak, R. H. (2023). Disturbo post-traumatico da stress. Le cliniche mediche del Nord America, 107(1), 85-99. https://doi.org/10.1016/j.mcna.2022.04.003
Commenti
I would expect that most PT\'s / manual therapist will remember at least one patient in the last 10 years with expressions of PTSD.
If I look back over my career, I remember several patients who must have had post-traumatic stress, although it went unrecognized at the time. I wish sometimes that I could treat them now, as I learned more about the topic.
I remember a woman talking about an accident in which she fractured her patella. She spoke about it in such emotional detail as if it happened yesterday, but the accident was 5 years ago. I wish I had thought of asking her something as: \"how did this accident impact your life?\"or \"Does this accident haunt you?\" \"Do you dream about your accident?\" She may have more nightmares than before the accident
Another example is a man with a shoulder luxation 3 weeks ago. He was kicked off his bicycle by 3 young guys. He had severe sweating, nervousness, and eyes that could not focus for a longer period of time (got restless). My own accident left me for a while left me with some post-traumatic symptoms suas increased anxiety, palpitations, and irregular heart (all gone now with the help of a well-versed and experienced body worker/cranio sacral therapist). An 81-year golf buddy of ours, an ex-marine from the Vietnam war, recognized only 4 years ago that his inability to stay for longer periods in the same place (he moved a lot over the years after the war; always in education in US army bases of the world), nightmares and bouts of anxiety, were all expressions of a severe post-traumatic stress syndrome. He is getting help in a Veterans hospital in a specialized group. At an IFOMPT Conference in Kopenhagen, Denmark around 1996, a lecture dealt with PTSD. We were warned not to repeat the mechanisms of an accident over and over again in history-taking. (what trauma work would do, is NOT necessarily repeating the mechanisms of the incident -\"what happened\", but guiding and encouraging patients to explore what/how they felt at the time and afterwards.
I recommend readers to explore
- {{ errore[0] }}

